
Herd Immunity and SARS-CoV-2:
Herd Immunity and SARS-CoV-2:
A Political Play in 7 Parts (if Parts=Lies)- Parts 5 & 6


Viral Variants and Selective Evolutionary Pressure
With regard to viral evolution, there is a delicate interplay between mutation and survival that must occur. Mutate too much, and the virus may lose its ability to be transmitted, function properly, and/or cause future infections, or it may become too lethal, extinguishing itself with the too-rapid death of its hosts. Mutate too little and prior immunity will prevent successful transmission and infection. So nature favors evolution of those viruses which can thread this mutation-needle to adapt to have some advantage. The evolutionary “goal” of a virus after all is to continue to propagate itself.
LIE 5: “Pandemic of the unvaccinated;” the unvaccinated alone are responsible for variants and keeping the pandemic going
This then brings up the discussion of variants and selective evolutionary pressure. Variants of any viral illness can evolve due to random mutations that occur during EVERY replication cycle. Given that viral illnesses infect an enormous quantity of host cells, during any given viral infection an individual is host to a substantial quantity of replication cycles. Meaning that variants can be produced with each individual infection, which are then able to replicate themselves as the individual infection progresses. This does not necessarily mean that each infection spreads new variants or that the new variants give the virus a survival advantage. It just means that the opportunity arises.
However, there are factors which can increase the likelihood that new variants possess these attributes. We previously covered that the likelihood of mutations occurring is different for any given virus, but any time a virus is able to replicate, it is capable of producing new variants that can escape previously induced immunity. If this escape mechanism gives the virus a survival advantage, the more likely it is to become more dominant or widespread. In this way evolutionary selective pressure is induced by prior infection or vaccination.1 This is a known principle in virology. If a given obstacle is presented to a virus (in this case prior immunity), this pressures the virus’ mutations to attempt to overcome this obstacle. The virus isn’t “consciously” problem-solving, but by the nature of its replication, it is advantageous to its survival imperative that its progeny can avoid immune response.
We uncover another lie being deployed on the public. The unvaccinated are not the sole reason that the pandemic continues; rather those who do not possess solid, durable immunity (even animals; see LIE #1) will allow virus replication and spread to continue. Unfortunately, mass vaccination with a “leaky” vaccine that presents the identical survival challenge to a rapidly replicating virus can selectively steer said virus to evolve more quickly to escape a narrowly focused immunity. The spike protein vaccine is like giving the virus a beginner level challenge. And viruses such as coronaviruses are experts at adaptation.2 3
In a recent paper, the burden of vaccine-resistant strains among vaccinated and unvaccinated cases was investigated.4 From February 2021 to June 2021 for unvaccinated cases, approximately 60% of infections were with non-resistant variants, such as alpha and epsilon, which was in contrast to vaccinated cases, whose average proportion of non-resistant variants was 27%. Overall, they found that 78% of those fully vaccinated were infected with resistant variants (such as delta). This period of time was before delta variant had become dominant. Combine this with recent studies regarding natural immunity outperforming vaccine-induced immunity for preventing reinfection.5
Conclusion: it is possible that the vaccinated are actually more responsible for propagating the pandemic with regard to the dominance of the delta variant. It has been shown that even vaccinated individuals may carry up to 251 times higher viral loads with delta vs. variants in early 2020, and that the difference was even higher when comparing viral loads of asymptomatic groups,6 implying greater chance for asymptomatic transmission with delta. A faster replication cycle for delta may account for this.7 When you consider that the narrowly-focused, vaccine-induced immunity selects against the alpha variant, it is understandable why delta variant comparatively would have more success infecting the vaccinated. These findings are logical when considered within the framework of selective evolutionary pressure.
Another recent paper8 modeling emergence and establishment of a vaccine-resistant strain further demonstrates this:
“The coincidence of a high number of vaccinated individuals and a high rate of transmission has two effects on the resistant strain. First, as mentioned previously, because the rate of transmission is high, the emerging resistant strain is not lost through genetic drift. Second, a high number of vaccinations creates a selective advantage of the resistant strain over the wild-type strain.” <Emphasis added>
And:
“…the highest risk of resistant strain establishment occurs when a large fraction of the population has already been vaccinated but the transmission is not controlled… the establishment of a resistant strain at that time may lead to serial rounds of resistant strain evolution with vaccine development playing catch up in the evolutionary arms race against novel strains.”
Again, it would seem that our “experts” threw established scientific principles and thinking out the window. And threw the unvaccinated under the bus. A convenient smokescreen/scapegoat/catchphrase for supposedly why their vaccines and protocols were not working.
Bottom line: “Pandemic of the unvaccinated" is false (further supported in charts and graphs in next installment). Worse, it’s a divisive, punitive phrase meant to mislead, marginalize, and incriminate. It is not founded in science.
Data has only further accumulated to support this since the time of first writing this (September/October 2021).
LIE 6: Ignoring the concept of durable immunity: comparing smallpox, poliovirus, or measles immunity to SARS-CoV-2
Many previous paragraphs relate to Requirement #3 for herd immunity against SARS-CoV-2. In fact, Lies #3-5 touch on why this requirement is not possible. Bottom line: the COVID-19 vaccines only confer partial immunity, which is in direct opposition to Requirement #3. And they knew in advance that this was true. Below is a more complete explanation.
Durable, solid immunity refers to an immune response that is sufficient to prevent the establishment of primary infection and shedding of mature virus particle (transmission) for decades or a lifetime.9 10 It is sometimes referred to as sterilizing immunity. This is contrasted with partial immunity, which allows for infection and transmission to occur while only possibly preventing severe disease. Intrinsic properties of a particular virus impact the probability and possibility for solid immunity, as does the immune response mounted against said virus/vaccine. As discussed, properties of SARS-CoV-2 that were known very early on argued against the probability of lifelong immunity to all future variants and certainly argued against it for spike protein vaccine-induced immunity. Yes, lifelong immunity may exist for strains closely related to that which prompted the immune response, however, with enough deviation from the original infecting strain, it is possible that cross-immunity will not provide enough protection to maintain herd immunity. Translation: at some point in the future, any given individual may likely become susceptible to another infection, just as what happens with the common cold or the flu. SARS-CoV-2 is not evolutionarily stable as compared to smallpox, poliovirus, or measles.
When the nature of SARS-CoV-2 is considered with respect to vaccine development, it was always a fool’s errand to expect that a vaccine which only confers immunity based on one arrangement of spike protein would impart solid immunity against a virus with such a likelihood for mutation and variant production, especially since for coronaviruses “the S1 subunit of the spike protein…is prone to high mutation rates as the virus evolves in host populations.”11 “In the case of SARS-CoV-2, mutations in S are most likely to confer fitness to the virus as it adapts to humans”12 and “adaptive processes could interfere with vaccine efficacy.” Additional quotes reiterating the same lessons learned from other previous SARS-CoV and MERS-CoV studies:
• A “concern is that for SARS-CoV escape from neutralization is driven by spike protein variability; thus, spike-dependent vaccine strategies might require multivalent approaches."13
• “For therapeutic antibody and vaccine design, it is critically important to develop or elicit broadly cross-reactive neutralizing antibodies (nAbs) that neutralize a broad range of antigenically disparate viruses…”14
• “Safety considerations and the degree of extensive diversity in antigenic variants are some of the potential reasons that limit coronavirus vaccine development. (13)
• “In general, vaccine development for pathogens with a high rate of antigenic changes in their surface antigens such as SARS-CoV is difficult and complicated due to the emergence of vaccine escape variants over time.”15
• “An ideal SARS vaccine should 1) elicit highly potent neutralizing antibody responses against a broad spectrum of viral strains; 2) induce protection against infection and transmission; and 3) be safe by not inducing any infection-enhancing antibodies or harmful immune or inflammatory responses.”16 (A CDC publication)
• “the nature of the rapid variation in the RNA virus increases the likelihood of immunologic escape, especially with regard to countermeasures directed at the RBD.”17 (RBD=receptor binding domain)
• “the antigenic variation in the S-protein between CoVs limits the breadth of cross protection against multiple emerging CoVs, and is especially true for S-protein only vaccines.”18
• “Vaccine development faces a series of potential concerns including reversion or recombination repair of attenuated vaccine strains, induction of immune-mediated enhancement of pathology, waning immune protection, lack of cross-protection for heterologous strains, and limited vaccine efficacy within senescent populations…SARS vaccines might fail to induce antibodies that protect from infection with divergent strains of SARS-CoV… possibly limiting the effectiveness of monotypic SARS-S vaccines.”19
• “The evolving molecular heterogeneity of SARS-CoV (11, 12, 21, 22) has raised concerns about the breadth and efficacy of protection with specific vaccine strains and the possible development of immune escape… the resistance of some S strains to Ab neutralization raises concerns about the ability of SARS-CoV vaccines to contain the spectrum of isolates in nature”20
• “One problem facing animal coronavirus vaccines has been strain variation among field isolates, leading to variable vaccine efficacy.”21
• “Ideally, drugs and vaccines should target relatively invariant, strongly constrained regions of the SARS-CoV-2 genome, to avoid drug resistance and vaccine evasion.”22
• “protection must be thorough enough to prevent NAb escape, a phenomenon inversely correlated with the number of immunogenic epitopes.”23
• “in the face of mounting evidence that coronaviruses are quite capable of shifting receptor affinity, an ability that would most assuredly place them outside of the prohibitory curtain of most nMAbs and perhaps of vaccines, it is becoming increasingly evident that development of therapeutic avenues and vaccines that target broader, more universally conserved alleles and a variety of loci across phylogenetic subclusters is of paramount importance, especially for emerging viruses that originate from highly heterogeneous pools of precursor zoonotic viruses.”24
The list could go on, but you get the picture. Hopefully this demonstrates the overwhelming acknowledgement of these limitations in the coronavirus vaccine literature. It was widely accepted that vaccine escape variants were likely and problematic, especially with spike-protein focused vaccines, meaning that partial immunity at best was also the overwhelming likelihood. In fact, one of the above studies from 2017 showed that “protection was incomplete,” since MERS infected all mice in both of the immunized groups. (15)
Further support regarding these known near-certainties comes from research regarding neutralizing antibodies (nAbs) as therapeutics (yes, monoclonal antibodies had been known for over a decade as possible effective treatments (12, 16); hmm quite the red flag once again, no? More on this another time). One study found that “all nAbs tested, including strain-specific or broadly reactive nAbs, selected for escape mutants.”(12) They questioned “if the RBD is generally not an ideal target for development of escape-resistant broadly neutralizing Abs against the SARS-CoV or any potential novel emerging CoVs.” In a different study25, “a single-amino-acid substitution (D480G) in their RBDs”(12) prevented neutralizing capability. Only ONE mutation. (Remember from Parts 3 & 4 how many variants abound?) Still other studies report that the spike protein is the part of coronaviruses most involved by mutations!26 27 28 (17) Example:
“S…becomes the most rapidly evolving protein, with most mutations located in the S1 domain and especially the receptor binding domain.” (26)
Selective evolutionary pressure will win every time, to use the language of which they are so fond. The phrases “planned obsolescence” or “kicking the can down the road” come to mind (plan for annual boosters anyone?).
The vaccines for smallpox, poliovirus, and measles use either live virus, inactivated (dead), or attenuated (weakened) live viruses, which allow the immune system to “see" the ENTIRE structure of each respective virus. This produces more complex, broad-based immunity which is more successful at producing solid immunity, especially when a virus is evolutionarily stable. It comes down to this: rather than only needing to sufficiently change one tiny portion of the virus to overcome prior immunity, multiple changes would be necessary to accomplish a similar result. The nature of probabilities makes the former “easier,” more likely, and consequently possibly arise faster than the latter. A bit like the difference between playing Twister after one spin vs. 10 spins.

What had been learned from SARS-CoV and MERS-CoV Vaccine Research?
However, it was also foolhardy to claim that durable, solid immunity would be possible in the face of previous, relevant data. Seventeen years of SARS-CoV research and nearly a decade of MERS-CoV research had never produced an approved vaccine against a coronavirus.29 30(14, 32) Only a handful had even progressed to Phase I or II human clinical trials before COVID.31 32 33 Yet we jumped to concurrently run Phase I/II and Phase II/III trials with a novel vaccine platform against a novel coronavirus after only a couple of months. Prior studies of vaccines for SARS-CoV (which is ~80% similar to SARS-CoV-2)34 showed that immune response wanes rapidly and significantly after as little as a few months from the time of last inoculation. One study title referred to “long-term immunity” as immune response at 1 and 4 months!35 Another study protocol involved a series of up to 3 boosters over 12 months (for a total of 4 shots), only to test the study animal with viral challenge 5 days after the final dose!36 In fact, of 27 SARS-CoV vaccine studies that actually utilized post-vaccine viral challenge, the majority (24 of 27) utilized a challenge timed only a few weeks (avg. 2-4 wks.) after inoculation (only 3 even looked at ~3 or 4 months!).37 Most studies also used animals that don’t adequately demonstrate the pathophysiology of SARS or MERS infections in humans and did not test heterologous strains or aged animals (12, 17, 26, 28). These limitations in study design are glaring obstacles. Proving something “effective” for such a narrow window, in young healthy animals that can’t even demonstrate severe or lethal outcomes anyway has quite limited translational value to real world scenarios— 1) Where immunity needs to be strong for long after the last dose; 2) Where it needs to hold up under challenge from the same strain and other strains; 3) Where it needs to be effective for those most at risk of severe illness and death (those over 65 and with co-morbidities were known for SARS and MERS too38).
Slight tangent, but needs mentioning as it ties back to the above critiques: Investigation of vaccine-enhanced disease (VED; aka vaccine-associated enhanced disease (VAED)), which is known to possibly be caused when immunity wanes (38), suffers from the same lack of looking long-term. All studies I found claiming a VED result, whether found or not found, only tested the animals within days or weeks of last inoculation. If you do not look where (AND WHEN) it’s most likely to occur, how can you expect to find it? OR maybe that’s the point. Publication bias is real.39
So perhaps the goal and intended protocol was to incorporate boosters indefinitely, closely approximating how we create and utilize annual flu shots (more on this in Lie #7). With most published study constructs testing vaccine candidates after only days to a month or two later, it would seem to imply that long term immunity was not even attempted, since perhaps escape-variant and waning immunity likelihood were understood. One of the two completed human clinical trials for a SARS vaccine candidate used three doses.(27) Another planned for a booster dose (3 shots) but the study was terminated without details why,40 while two of three MERS human clinical trials used 3 doses. Add to this the inconsistent immunogenicity produced for neutralizing antibodies (those things we’ve repeatedly been told are so important, but “correlates of protection for MERS-CoV are currently unknown” as of July 2020!) for the MERS candidates— nABs were detected only in the low-dose group (1 of 5 participants) and high-dose group (four of nine [44%]) with 0 of 8 in the intermediate group for one trial; and another trial showed nABs were detected only in 34 (50%) of 68 participants!(28) Do they really expect people to believe that their goal was to make vaccines which would be completed in one or two doses for a lifetime of immunity, in the face of all of this evidence to the contrary?
Exceptionally incompetent or lying, which is it?
How about this for an answer from Pfizer:
“Waning effectiveness and an increased number of infections 6–12 months after the second dose—along with the potential need for booster doses—was expected given that lower neutralising antibody titres during this time period have been observed in immunogenicity studies.34, 35, 36 Waning has been observed for both mRNA-based (Pfizer–BioNTech and Moderna) COVID-19 vaccines,26, 27 and is consistent with studies of other coronaviruses.37”(55)
Precisely catches them in the lie. But really? Only one previous coronavirus article to cite and from 1990?! I’ve shown a glimpse of how much is actually out there to guide their decisions! Even when letting the truth leak out, they still try to cover it up or spin it. But this explains so much:
And:

Just imagine how crucially important parts that are study design, data interpretation and writing of the report can be manipulated. Hiding the truth in plain sight is not integrity.
Mini Bottom Line: SARS and MERS vaccine candidate research has not shown consistent results with respect to durability, immunogenicity, or safety across a wide variety of different vaccine platforms, target antigens, study designs, study animals, viral challenges, and different adjuvants. While some important pitfalls had been identified, much remained to be understood, most of all how these would perform in humans.
Additionally very few studies using senescent animals have been conducted. Those few that have showed a less durable response upon viral challenge after vaccination compared to young animals.(14) 41 The population that needs it most has shown the least benefit. Many studies also found safety concerns42 43 44 45 46 47 (27) and even concluded that caution would be advised for their application to human populations.(14) 48 49
Does it seem reasonable to assume that SARS-CoV-2 vaccine-induced immunity would be different from results found doing research on closely related virus vaccines? Or is it perhaps more appropriate to assume that limitations encountered for decades would likely persist until proven otherwise? After all what’s the point of accumulating vast amounts of research only to ignore their findings and not apply them to similar future scenarios on the basis of hoping for the contrary? This is either an unscientific approach or not being transparent.
So how about Pfizer, Moderna, and J&J clinical trials data?
When considering their own 2020 clinical trials data50 51 52 53 54 55 (which assessed only up to 2 months afterward), all three vaccines currently available in the U.S. had breakthrough cases, even moderate to severe illness and hospitalization. Their explicit aims even acknowledge the known limitations, when you consider that they chose to assess reduction in symptoms (“prevention of symptomatic COVID”) as the successful metric. We’ve established that a vaccine which only reduces symptoms implies only partial immunity and partial immunity implies they do not stop infection or transmission. It’s similar to the point from above regarding data published for SARS and MERS vaccine research: if you set up the experiment with the greatest chance to show positive results, you can leave out questions that might reflect poorly. Or just say To Be Continued. To be clear, the protocol for clinical trials dictates that they must choose these metrics before conducting the clinical trial, since this is part of the registration/application process. With decades of research at their disposal, they could certainly make the shrewd, calculated decision to set their trial up best to “succeed.”
For example:
“a third clinical trial design could focus on those at highest risk for severe infection. Such a study would more easily discern vaccine effectiveness since the primary outcome would compare morbidity and death between vaccine and placebo. However, those at highest risk for severe disease including the elderly and those with underlying illness such as cardiac, pulmonary, and renal disease may limit vaccine immune responsiveness.”(55)
If they truly were attempting to prevent infection and transmission, or severe illness and death, wouldn’t these have been the measured outcomes? I argue that this choice was made because it was the lowest, fastest bar to clear, allowing them to appear to check some efficacy boxes with the goal to rush these to post-authorization study. Especially while the pandemic was still in full swing, with a virus-naive population. Admitted limitations of prior SARS or MERS vaccine development, and hence advancement, have been that human clinical trials suffer from post-vaccination challenge.(12, 28) 56 57 It’s been stated that:
"Human vaccine effectiveness studies will only be possible in the context of SARS re-emergence…Re-emergence of SARS now looms as an uncertain possibility. Maintaining interest in vaccine development against that uncertainty becomes an ongoing challenge.”(28)
“The commercial viability of developing a vaccine for SARS-CoV will ultimately depend on whether the virus re-emerges in the near future.”
“Early clinical studies…have been carried out, but it is difficult to push the clinical trials of these candidate vaccines and therapeutics forwards owing to a lack of SARS-CoV-infected subjects and insufficient financial support. Thus, most big pharmaceutical companies have no interest in developing SARS vaccines and therapeutics because of the concern of profitability.”(56)
“Although several potential therapies have been identified with SARS and MERS in animal and in vitro models, human clinical trials remain lacking, hindering the advancement of these potential countermeasures.”58
“A major reason for the lack of approved and commercially available vaccines or therapeutic agents against these CoVs might be the relative lack of interest among the pharmaceutical companies.13 These are outbreak scenarios: the demand for drugs or vaccines lasts only for a period while the outbreak lasts. The number of affected people will also be a small proportion of the global drug and vaccine market. So by the time a new drug or vaccine is developed, there might not be any patients for clinical trials and also no meaningful market for newly discovered drugs.”59
“…efficacy data from human clinical trials are lacking but are needed to move these potential countermeasures forward.”60
Hmmm…how many new billionaires were minted last year? They sure solved that problem. And that pesky no re-emergence problem too.
With this understanding they knew that they may have only a limited window (SARS and MERS each subsided within ~ 1 year, Zika epidemic 2015-2016 resolved before vaccine field trials could be done61) during which to disseminate, administer, and collect data on the vaccine performance. An article in Nature even states,"The NIAID argues that the risk of delaying the advancement of vaccines is much higher than the risk of causing illness in healthy volunteers…”62 From someone (Dr. Fauci) who in 2012 reflected as follows on a hypothetical situation:
Imagine “an important gain-of-function experiment involving a virus with serious pandemic potential is performed…what if that scientist becomes infected with the virus, which leads to an outbreak and ultimately triggers a pandemic?…as indeed I have said – that the benefits of such experiments and the resulting knowledge outweigh the risks…the time it takes to engage in such a dialog <about whether these experiments should have been performed in the first place.> could potentially delay or even immobilize the conduct of certain important experiments and the publication of valuable information that could move the field forward for the good of public health.”63
Do you really think that same person would miss this opportunity to “move the field forward” in coronavirus vaccine data generation, just because it might be questionably unethical or dangerous? He is 81 after all. Better get while the gettin’s good.
Or maybe I’ve just seen “Jurassic Park” too many times:
Dr. Ian Malcolm :…to accomplish something as fast as you could, and before you even knew what you had, you patented it, and packaged it, and slapped it on a plastic lunchbox, and now [bangs on the table] you're selling it, you wanna sell it.

Dr. Ian Malcolm : John, the kind of control you're attempting simply is... it's not possible. If there is one thing the history of evolution has taught us it's that life will not be contained. Life breaks free, it expands to new territories and crashes through barriers, painfully, maybe even dangerously, but, uh…well, there it is.

Dr. Ian Malcolm : Gee, the lack of humility before nature that's being displayed here, uh... staggers me.
Here’s a thought experiment. It comes to mind that perhaps some measures were undertaken in order to draw out this window with the clever cover of “saving lives.” While lockdowns, closing schools and businesses, masks, etc. were supposed to “flatten the curve,” this conveniently also widened/lengthened the curve, giving more time to conduct their experiments. Then use a leaky vaccine to allow spread while telling everyone that they can’t catch it or spread it. Then suspend nationally tracking breakthrough cases that don’t result in hospitalization or death (CDC as of May 1, 2021, more on this next time). Kind of makes the perfect conditions to NOT end the pandemic. Makes you wonder.
And I say deploy their experiments because that is exactly what they are. It’s acknowledged in their Vaccine and Related Biological Products Advisory Committee (VRBPAC) EUA meeting documents from December 2020 64that “a larger number of individuals at high risk of COVID-19 and higher attack rates would be needed” in order to evaluate whether the vaccines have any mortality benefit. And data was “limited to assess the effect of the vaccine against transmission.” “Additional evaluations including data from clinical trials and from vaccine use post-authorization will be needed.” Additionally from the FDA revised EUA letter65 dated September 22, 2021:
“Pfizer Inc. will conduct post-authorization observational studies to evaluate the association between Pfizer-BioNTech COVID-19 Vaccine and a pre- specified list of adverse events of special interest, including myocarditis and pericarditis, along with deaths and hospitalizations, and severe COVID-19. The study population should include individuals administered the authorized Pfizer-BioNTech COVID-19 Vaccine under this EUA in the general U.S. population (12 years of age and older), individuals that receive a booster dose, populations of interest such as healthcare workers, pregnant women, immunocompromised individuals, subpopulations with specific comorbidities.” <emphasis added>
Did participants know they volunteered to be part of these post-authorization studies? Were they told this would be the case? Multiple retrospective observational studies have been conducted since the vaccination program has been rolled out and some even registered as clinical trials.66 67 68 One clinical trial from Moderna estimates 50,000,000 “participants” who received the shot under EUA. The design of these studies, as retrospective observational or public health surveillance, allows the use of patient data without the need for informed consent by the Institutional Review Boards (IRBs) (who oversees biomedical research involving human subjects to assure, both in advance and by periodic review, that appropriate steps are taken to protect the rights and welfare of humans participating as subjects in the research.) From one such vaccine post-auth. retrospective observational clinical trial paper:
“The study protocol was reviewed and approved by the KPSC institutional review board, which waived requirement for informed consent…”(54)
And one from Michigan (ClinicalTrials.gov Identifier: NCT04912700):
“Written informed consent requirement was waived due to the retrospective nature of this study.”69
I argue that this is a devious, slick work-around for the normal informed consent that would be required for these vaccines to be researched in the conventional way. That they specifically admit in their Dec. 2020 VRBPAC EUA meeting documents and the many updated iterations of FDA EUA letters that all of these outcomes would require post-auth. investigation means that they knew beforehand that the construct would be retrospective observational studies, obviating the usual informed consent necessary.
A final thought concerning this. With the foreknowledge and planning that post-auth. studies would investigate such a wide variety of questions regarding vaccine performance, isn’t it possible that early treatment was kept quiet, discounted, and even blatantly tanked in order to assure that the data collected post-auth. for these studies would not be confounded by such hugely significant variables? Imagine how widespread the use of early treatment would have been if it were marketed at even a fraction of how the vaccines have been. Imagine how difficult (that is to say likely impossible) it would be to separate out the benefit of early treatment from effectiveness of the vaccine. All of their post-auth. studies would at best require significant disclaimers or at worse be junk. What better way to keep their data as clean as possible than to pretend there are no treatments until someone is so sick as to need hospitalization? And at this point, require the hospitals to only utilize a select few treatments (rewarding them if they follow approved protocol with financial compensation and liability protection, but negating liability protection if any deviation from the protocol occurs) so as to keep the data cleaner yet again. Maybe they changed the definition of RCT… retrospective controlled trials.
I admit that this sounds like wild-eyed speculation (even though it so nicely explains a lot of the head-scratchingly wrong turns for the past two years). Maybe I could leave it at that, except for this from the KPSC Pfizer-funded study:
“ There will be no exclusion criteria for the cohort design, however patients will be censored for receiving any other newly licensed or investigational SARS-CoV-2 vaccine or COVID-19 prophylactic agent other than Pfizer's COVID-19 vaccine. Patients will also be censored if the event (hospitalization, ED encounter, etc.) occurs within certain time windows from vaccination date.”70
And this from the Phase 1/2/3 Pfizer BioNTech clinical trial:
"Exclusion criteria:
• Receipt of medications intended to prevent COVID 19…
• Participation in other studies involving study intervention within 28 days prior to study entry through and including 6 months after the last dose of study intervention, with the exception of non-Pfizer interventional studies for prevention of COVID 19, which are prohibited throughout study participation.”71
And this:
The trial was submitted June 10, 2020, began July 1, 2020, and the end date was Dec. 1, 2020, just days from Pfizer’s vaccine EUA initial approval. Coincidence?
And this:
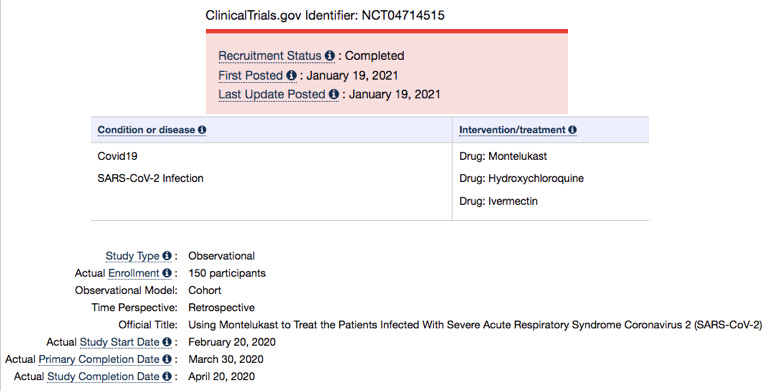
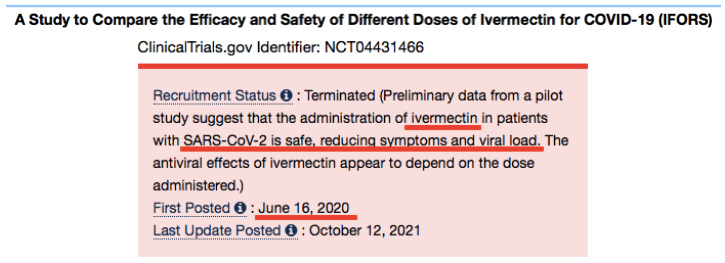
Study in China and Pakistan on Ivermectin, Hydroxychloroquine, and Montelukast from Feb. 2020, ended April 2020, no results or paper to be found yet…
It doesn’t require a large stretch of the imagination to put pieces together in this way. Simply put yourself in the mindset of a diabolical, egomaniacal, octogenarian, puppet master bureaucrat hell-bent on getting his Nobel prize and throw in the wildest dreams of a profits-driven, liability-protected pharma merchant. Voila! Perfect way to control for key variables in a worldwide experiment and generate billions for years to come.
As Stefan Oelrich president of Bayer’s Pharmaceutical Division said at the World Health Summit (Berlin, October 24-26, 2021):
“ultimately the mRNA vaccines are an example for that cell and gene therapy. I always like to say: if we had surveyed two years ago in the public – ‘would you be willing to take a gene or cell therapy and inject it into your body?’ – we probably would have had a 95% refusal rate. I think this pandemic has also opened many people’s eyes to innovation in a way that was maybe not possible before.”72 73
And as Pfizer CEO Albert Bourla admitted in February 2021 that Israel is “the world's lab”74, then another Pfizer executive, chief scientific officer Philip Dormitzer, in September 2021 stated that Israel was “a sort of laboratory where we could see the effect”75 of their vaccines. Just understand when they said Israel, they meant the world.
What does Tom Cruise say again about Jack Nicholson’s character in “A Few Good Men”? “I think he wants to say it. I think he’s pissed off that he’s gotta hide from this…<imitating Jessup> He eats breakfast 300 yards away…”.

The more they talk, the more they revel in what they’ve done, the more they’re led exactly where they’re dying to go. They can’t help themselves.
Bottom line: They knew in advance that the vaccines were not shown to prevent infection or moderate and severe illness (even within 7 weeks of being “fully vaccinated” when protection is strongest), and they knew in advance that they did not determine the prevention of transmission or prevention of death.
They most assuredly knew what they did not know. And what they did know. And how to use both to their advantage.
Yet, the opposite was repeatedly the claim made to the public in late 2020 and into 2021, when they said “Protect those around you,” “Protect grandma,” “Protect your community.” Such “leaky” vaccines that provide only partial immunity serve to establish a breeding ground for variants and viral propagation (perhaps by design?). Requirement #3 is not met for SARS-CoV-2 to achieve herd immunity. Again they knew this from early on and it has only been further confirmed with each passing month.
Flint J, Racaniello VR, Rall GF, Hatziioannou T, Skalka AM. Principles of Virology. 5th ed. ASM Press; 2020.
Pyrc K, Dijkman R, Deng L, et al. Mosaic structure of human coronavirus NL63, one thousand years of evolution. J Mol Biol. 2006;364(5):964-973. doi:10.1016/j.jmb.2006.09.074 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7094706/
Pachetti, M., Marini, B., Benedetti, F. et al. Emerging SARS-CoV-2 mutation hot spots include a novel RNA-dependent-RNA polymerase variant. J Transl Med 18, 179 (2020). https://doi.org/10.1186/s12967-020-02344-6 https://link.springer.com/article/10.1186/s12967-020-02344-6
Servellita V, Sotomayor-Gonzalez A, Gliwa AS, Torres E, Brazer N, Zhou A, Hernandez KT, Sankaran M, Wang B, Wong D, Wang C, Zhang Y, Reyes KR, Glasner D, Deng X, Streithorst J, Miller S, Frias E, Rodgers M, Cloherty G, Hackett Jr. J, Philip S, Topper S, Sachdev D, Chiu CY. Predominance of antibody-resistant SARS-CoV-2 variants in vaccine breakthrough cases from the San Francisco Bay Area, California. medRxiv 2021.08.19.21262139; doi: https://doi.org/10.1101/2021.08.19.21262139 https://www.medrxiv.org/content/10.1101/2021.08.19.21262139v2.full#F1
Gazit S, Shlezinger R, Perez G, Lotan R, Peretz A, Ben-Tov A, Cohen D, Muhsen K, Chodick G, Patalon T. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections. medRxiv 2021.08.24.21262415; doi:https:// doi.org/10.1101/2021.08.24.21262415.https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1
Nguyen Van Vinh Chau et al. An observational study of breakthrough SARS-CoV-2 Delta variant infections among vaccinated healthcare workers in Vietnam. EClinicalMedicine, Volume 41, 2021,101143,ISSN 2589-5370 https://www.sciencedirect.com/science/article/pii/S2589537021004235
Baisheng Li et al. Viral infection and transmission in a large, well-traced outbreak caused by the SARS-CoV-2 Delta variant. medRxiv 2021.07.07.21260122; doi: https://doi.org/10.1101/2021.07.07.21260122 https://www.medrxiv.org/content/10.1101/2021.07.07.21260122v2.full-text
Rella, S.A., Kulikova, Y.A., Dermitzakis, E.T. et al. Rates of SARS-CoV-2 transmission and vaccination impact the fate of vaccine-resistant strains. Sci Rep 11, 15729 (2021). https://doi.org/10.1038/s41598-021-95025-3. https://www.nature.com/articles/s41598-021-95025-3#citeas
Read AF, Baigent SJ, Powers C, Kgosana LB, Blackwell L, Smith LP, Kennedy DA, Walkden-Brown SW, Nair VK. Imperfect Vaccination Can Enhance the Transmission of Highly Virulent Pathogens. PLoS Biol. 2015 Jul 27;13(7):e1002198. doi: 10.1371/journal.pbio.1002198. PMID: 26214839; PMCID: PMC4516275. https://pubmed.ncbi.nlm.nih.gov/26214839/
Boodhoo, N., Gurung, A., Sharif, S. et al. Marek’s disease in chickens: a review with focus on immunology. Vet Res 47, 119 (2016). https://doi.org/10.1186/s13567-016-0404-3 https://veterinaryresearch.biomedcentral.com/articles/10.1186/s13567-016-0404-3
Ruan YJ, Wei CL, Ee AL, et al. Comparative full-length genome sequence analysis of 14 SARS coronavirus isolates and common mutations associated with putative origins of infection [published correction appears in Lancet. 2003 May 24;361(9371):1832]. Lancet. 2003;361(9371):1779-1785. doi:10.1016/s0140-6736(03)13414-9 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7140172/
Dearlove B, Lewitus E, Bai H, Li Y, Reeves DB, Joyce MG, Scott PT, Amare MF, Vasan S, Michael NL, Modjarrad K, Rolland M. A SARS-CoV-2 vaccine candidate would likely match all currently circulating variants. Proceedings of the National Academy of Sciences Sep 2020, 117 (38) 23652-23662; DOI: 10.1073/pnas.2008281117. https://www.pnas.org/content/117/38/23652?ijkey=646a60cbd25397bf82b3d80f6d715fc2ae30e162&keytype2=tf_ipsecsha
Graham RL, Donaldson EF, Baric RS. A decade after SARS: strategies for controlling emerging coronaviruses. Nat Rev Microbiol. 2013;11(12):836-848. doi:10.1038/nrmicro3143. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5147543/
Sui J, Deming M, Rockx B, et al. Effects of human anti-spike protein receptor binding domain antibodies on severe acute respiratory syndrome coronavirus neutralization escape and fitness. J Virol. 2014;88(23):13769-13780. doi:10.1128/JVI.02232-14 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4248992/
Khalaj-Hedayati A. Protective Immunity against SARS Subunit Vaccine Candidates Based on Spike Protein: Lessons for Coronavirus Vaccine Development. J Immunol Res. 2020;2020:7201752. Published 2020 Jul 18. doi:10.1155/2020/7201752. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7368938/
Jiang S, He Y, Liu S. SARS Vaccine Development. Emerging Infectious Diseases. 2005;11(7):1016-1020. doi:10.3201/eid1107.050219. https://wwwnc.cdc.gov/eid/article/11/7/05-0219_article
Jiaming L, Yanfeng Y, Yao D, et al. The recombinant N-terminal domain of spike proteins is a potential vaccine against Middle East respiratory syndrome coronavirus (MERS-CoV) infection. Vaccine. 2017;35(1):10-18. doi:10.1016/j.vaccine.2016.11.064. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7115548/
Tse Longping V., Meganck Rita M., Graham Rachel L., Baric Ralph S. The Current and Future State of Vaccines, Antivirals and Gene Therapies Against Emerging Coronaviruses. Frontiers in Microbiology. Volume 11. April 24, 2020. https://www.frontiersin.org/articles/10.3389/fmicb.2020.00658/full
Deming D, Sheahan T, Heise M, Yount B, Davis N, et al. (2006) Vaccine efficacy in senescent mice challenged with recombinant SARS-CoV bearing epidemic and zoonotic spike variants. PLoS Med 3(12): e525. doi:10.1371/ journal.pmed.0030525. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1716185/pdf/pmed.0030525.pdf
Yang ZY, Werner HC, Kong WP, et al. Evasion of antibody neutralization in emerging severe acute respiratory syndrome coronaviruses. Proc Natl Acad Sci U S A. 2005;102(3):797-801. doi:10.1073/pnas.0409065102. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC545557/
Peiris JS, Guan Y, Yuen KY. Severe acute respiratory syndrome. Nat Med. 2004;10(12 Suppl):S88-S97. doi:10.1038/nm1143 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7096017/
van Dorp L, Acman M, Richard D, Shaw LP, Ford CE, Ormond L, Owen CJ, Pang J, Tan CCS, Boshier FAT, Torres Ortiz A, Balloux F. Emergence of genomic diversity and recurrent mutations in SARS-CoV-2. Infection, Genetics and Evolution, Volume 83, 2020, 104351, ISSN 1567-1348, https://doi.org/10.1016/j.meegid.2020.104351. https://www.sciencedirect.com/science/article/pii/S1567134820301829
Schindewolf C, Menachery VD. Middle East Respiratory Syndrome Vaccine Candidates: Cautious Optimism. Viruses. 2019 Jan 17;11(1):74. doi: 10.3390/v11010074. PMID: 30658390; PMCID: PMC6356267. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6356267/
Graham RL, Baric RS. Recombination, reservoirs, and the modular spike: mechanisms of coronavirus cross-species transmission. J Virol. 2010;84(7):3134-3146. doi:10.1128/JVI.01394-09. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2838128/
Sui J, Li W, Roberts A, et al. Evaluation of human monoclonal antibody 80R for immunoprophylaxis of severe acute respiratory syndrome by an animal study, epitope mapping, and analysis of spike variants. J Virol. 2005;79(10):5900-5906. doi:10.1128/JVI.79.10.5900-5906.2005. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1091676/
Cheng VC, Lau SK, Woo PC, Yuen KY. Severe acute respiratory syndrome coronavirus as an agent of emerging and reemerging infection. Clin Microbiol Rev. 2007;20(4):660-694. doi:10.1128/CMR.00023-07. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2176051/
Martinez IL, Llinás DT, Romero MB, Salazar LM (2020) High Mutation Rate in SARS-CoV-2: Will It Hit Us the Same Way Forever?. J Infect Dis Epidemiol 6:176. doi.org/10.23937/2474-3658/1510176. https://clinmedjournals.org/articles/jide/journal-of-infectious-diseases-and-epidemiology-jide-6-176.php?jid=jide
Severe Acute Respiratory Syndrome (SARS): A Year in Review. Danuta M. Skowronski, Caroline Astell, Robert C. Brunham, Donald E. Low, Martin Petric, Rachel L. Roper, Pierre J. Talbot, Theresa Tam, Lorne Babiuk. Annual Review of Medicine. 2005, 56:1,357-381. https://www.annualreviews.org/doi/10.1146/annurev.med.56.091103.134135?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub++0pubmed
Badgujar KC, Badgujar VC, Badgujar SB. Vaccine development against coronavirus (2003 to present): An overview, recent advances, current scenario, opportunities and challenges. Diabetes Metab Syndr. 2020;14(5):1361-1376. doi:10.1016/j.dsx.2020.07.022. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7371592/
Dhama K, Sharun K, Tiwari R, et al. COVID-19, an emerging coronavirus infection: advances and prospects in designing and developing vaccines, immunotherapeutics, and therapeutics. Hum Vaccin Immunother. 2020;16(6):1232-1238. doi:10.1080/21645515.2020.1735227. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7103671/
Martin JE, Louder MK, Holman LA, et al. A SARS DNA vaccine induces neutralizing antibody and cellular immune responses in healthy adults in a Phase I clinical trial. Vaccine. 2008;26(50):6338-6343. doi:10.1016/j.vaccine.2008.09.026 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2612543/
Folegatti PM, Bittaye M, Flaxman A, et al. Safety and immunogenicity of a candidate Middle East respiratory syndrome coronavirus viral-vectored vaccine: a dose-escalation, open-label, non-randomised, uncontrolled, phase 1 trial [published correction appears in Lancet Infect Dis. 2020 May 12;:] [published correction appears in Lancet Infect Dis. 2020 Jun 8;:]. Lancet Infect Dis. 2020;20(7):816-826. doi:10.1016/S1473-3099(20)30160-2 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7172901/
Phase I/IIa, Open-label, Dose Ranging Study to Evaluate the Safety, Tolerability and Immunogenicity of GLS-5300, Administered ID Followed by CELLECTRA® 2000 (Electroporation, EP). Aug. 2018-Apr. 2020. https://clinicaltrials.gov/ct2/show/NCT03721718
Bano, I, Sharif, M, Alam, S. Genetic drift in the genome of SARS COV-2 and its global health concern. J Med Virol. 2021; 94: 88- 98. https://doi.org/10.1002/jmv.27337 https://onlinelibrary.wiley.com/doi/10.1002/jmv.27337
Du L, Zhao G, He Y, et al. Receptor-binding domain of SARS-CoV spike protein induces long-term protective immunity in an animal model. Vaccine. 2007;25(15):2832-2838. doi:10.1016/j.vaccine.2006.10.031. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7115660/
Du L, Zhao G, He Y, et al. Receptor-binding domain of SARS-CoV spike protein induces long-term protective immunity in an animal model. Vaccine. 2007;25(15):2832-2838. doi:10.1016/j.vaccine.2006.10.031 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7115660/
Tse Longping V., Meganck Rita M., Graham Rachel L., Baric Ralph S. The Current and Future State of Vaccines, Antivirals and Gene Therapies Against Emerging Coronaviruses. Frontiers in Microbiology. Volume 11. April 24, 2020. https://www.frontiersin.org/articles/10.3389/fmicb.2020.00658/full
Totura AL, Bavari S. Broad-spectrum coronavirus antiviral drug discovery. Expert Opin Drug Discov. 2019;14(4):397-412. doi:10.1080/17460441.2019.1581171 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7103675/
Joober R, Schmitz N, Annable L, Boksa P. Publication bias: what are the challenges and can they be overcome?. J Psychiatry Neurosci. 2012;37(3):149-152. doi:10.1503/jpn.120065. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3341407/
Schindewolf C, Menachery VD. Middle East Respiratory Syndrome Vaccine Candidates: Cautious Optimism. Viruses. 2019;11(1):74. Published 2019 Jan 17. doi:10.3390/v11010074 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6356267/
Bolles M, Deming D, Long K, et al. A double-inactivated severe acute respiratory syndrome coronavirus vaccine provides incomplete protection in mice and induces increased eosinophilic proinflammatory pulmonary response upon challenge. J Virol. 2011;85(23):12201-12215. doi:10.1128/JVI.06048-11 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3209347/
Enjuanes L, Dediego ML, Alvarez E, Deming D, Sheahan T, Baric R. Vaccines to prevent severe acute respiratory syndrome coronavirus-induced disease. Virus Res. 2008;133(1):45-62. doi:10.1016/j.virusres.2007.01.021 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2633062/
Su, S., Du, L. & Jiang, S. Learning from the past: development of safe and effective COVID-19 vaccines. Nat Rev Microbiol 19, 211–219 (2021). https://doi.org/10.1038/s41579-020-00462-y https://www.nature.com/articles/s41579-020-00462-y
Munoz FM, Cramer JP, Dekker CL, et al. Vaccine-associated enhanced disease: Case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2021;39(22):3053-3066. doi:10.1016/j.vaccine.2021.01.055 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7901381/
Wang J, Zand MS. The potential for antibody-dependent enhancement of SARS-CoV-2 infection: Translational implications for vaccine development. J Clin Transl Sci. 2020;1-4. Published 2020 Apr 13. doi:10.1017/cts.2020.39. ncbi.nlm.nih.gov/pmc/articles/PMC7274027/
Lyons-Weiler J. Pathogenic priming likely contributes to serious and critical illness and mortality in COVID-19 via autoimmunity. J Transl Autoimmun. 2020;3:100051. Published 2020 Apr 9. doi:10.1016/j.jtauto.2020.100051 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7142689/
Smatti MK, Al Thani AA, Yassine HM. Viral-Induced Enhanced Disease Illness. Front Microbiol. 2018;9:2991. Published 2018 Dec 5. doi:10.3389/fmicb.2018.02991 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6290032/
Tong TR. Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV). Perspect Med Virol. 2006;16:43-95. doi:10.1016/S0168-7069(06)16004-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7114587/
Tseng CT, Sbrana E, Iwata-Yoshikawa N, Newman PC, Garron T, Atmar RL, Peters CJ, Couch RB. Immunization with SARS coronavirus vaccines leads to pulmonary immunopathology on challenge with the SARS virus. PLoS One. 2012;7(4):e35421. doi: 10.1371/journal.pone.0035421. Epub 2012 Apr 20. Erratum in: PLoS One. 2012;7(8). doi:10.1371/annotation/2965cfae-b77d-4014-8b7b-236e01a35492. PMID: 22536382; PMCID: PMC3335060. https://pubmed.ncbi.nlm.nih.gov/22536382/
FACT SHEET FOR HEALTHCARE PROVIDERS ADMINISTERING VACCINE (VACCINATION PROVIDERS) EMERGENCY USE AUTHORIZATION (EUA) OF THE JANSSEN COVID-19 VACCINE TO PREVENT CORONAVIRUS DISEASE 2019 (COVID-19). https://www.fda.gov/media/146304/download
FACT SHEET FOR HEALTHCARE PROVIDERS ADMINISTERING VACCINE (VACCINATION PROVIDERS) EMERGENCY USE AUTHORIZATION (EUA) OF THE MODERNA COVID-19 VACCINE TO PREVENT CORONAVIRUS DISEASE 2019 (COVID-19). Updated July 27, 2021. http://web.archive.org/web/20210727193605/https://www.fda.gov/media/144637/download
Baden LR et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N Engl J Med 2021; 384:403-416. Feb. 4, 2021. Published online Dec. 30, 2020. DOI: 10.1056/NEJMoa2035389 https://www.nejm.org/doi/full/10.1056/nejmoa2035389
FACT SHEET FOR HEALTHCARE PROVIDERS ADMINISTERING VACCINE (VACCINATION PROVIDERS) EMERGENCY USE AUTHORIZATION (EUA) OF THE PFIZER-BIONTECH COVID-19 VACCINE TO PREVENT CORONAVIRUS DISEASE 2019 (COVID-19). Updated July 25, 2021. http://web.archive.org/web/20210725062306/https://www.fda.gov/media/144413/download
Pollack FP et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med 2020; 383:2603-2615. Dec. 31, 2020. Published online Dec. 10, 2020. DOI: 10.1056/NEJMoa2034577. https://www.nejm.org/doi/full/10.1056/nejmoa2034577
Vaccines and Related Biological Products Advisory Committee December 10, 2020 Presentation - BNT162b2 Vaccine Candidate Against COVID-19 https://www.fda.gov/media/144325/download
Maslow JN. Vaccines for emerging infectious diseases: Lessons from MERS coronavirus and Zika virus. Hum Vaccin Immunother. 2017;13(12):2918-2930. doi:10.1080/21645515.2017.1358325 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5718785/
Du L, He Y, Zhou Y, Liu S, Zheng BJ, Jiang S. The spike protein of SARS-CoV--a target for vaccine and therapeutic development. Nat Rev Microbiol. 2009;7(3):226-236. doi:10.1038/nrmicro2090. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2750777/
Song Z, Xu Y, Bao L, et al. From SARS to MERS, Thrusting Coronaviruses into the Spotlight. Viruses. 2019;11(1):59. Published 2019 Jan 14. doi:10.3390/v11010059 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6357155/
Kuldeep Dhama, Khan Sharun, Ruchi Tiwari, Maryam Dadar, Yashpal Singh Malik, Karam Pal Singh & Wanpen Chaicumpa (2020) COVID-19, an emerging coronavirus infection: advances and prospects in designing and developing vaccines, immunotherapeutics, and therapeutics, Human Vaccines & Immunotherapeutics, 16:6, 1232-1238, DOI: 10.1080/21645515.2020.1735227.https://www.tandfonline.com/doi/full/10.1080/21645515.2020.1735227
de Wit E, van Doremalen N, Falzarano D, Munster VJ. SARS and MERS: recent insights into emerging coronaviruses. Nat Rev Microbiol. 2016;14(8):523-534. doi:10.1038/nrmicro.2016.81 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7097822/
Jamrozik E, Selgelid MJ. COVID-19 human challenge studies: ethical issues. Lancet Infect Dis 2020; 20: e198–203. Published Online May 29, 2020. https://doi.org/10.1016/ S1473-3099(20)30438-2 https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30438-2/fulltext
Jiang S. Don’t rush to deploy COVID-19 vaccines and drugs without sufficient safety guarantees. Nature 579, 321 (2020) .doi: https://doi.org/10.1038/d41586-020-00751-9 https://www.nature.com/articles/d41586-020-00751-9
Fauci AS. Research on highly pathogenic H5N1 influenza virus: the way forward. mBio. 2012;3(5):e00359-12. Published 2012 Nov 1. doi:10.1128/mBio.00359-12 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3484390/
Vaccines and Related Biological Products Advisory Committee Meeting December 10, 2020 FDA Briefing Document Pfizer-BioNTech COVID-19 Vaccine https://www.fda.gov/media/144245/download
FDA Pfizer-BioNTech COVID-19 vaccine EUA letter of authorization. Sept. 22, 2021. http://web.archive.org/web/20210923042939/https://www.fda.gov/media/150386/download
Tartof SY, Slezak JM, Fischer H, et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study. Lancet. 2021;398(10309):1407-1416. doi:10.1016/S0140-6736(21)02183-8 https://pubmed.ncbi.nlm.nih.gov/34619098/
Post-Marketing Safety of SARS-CoV-2 mRNA-1273 Vaccine in the US: Active Surveillance, Signal Refinement and Self-Controlled Risk Interval (SCRI) Signal Evaluation in HealthVerity. July 6, 2021. https://clinicaltrials.gov/ct2/show/NCT04958954?term=severe+acute+respiratory+syndrome&type=Obsr&draw=2
Gazit S, Shlezinger R, Perez G, Lotan R, Peretz A, Ben-Tov A, Cohen D, Muhsen K, Chodick G, Patolon T. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections. medRxiv 2021.08.24.21262415; doi: https://doi.org/10.1101/2021.08.24.21262415 https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full
Bahl A et al. Vaccination reduces need for emergency care in breakthrough COVID-19 infections: a multicenter cohort study. The Lancet Regional Health. Vol 4, Dec 1, 2021. Published online Sept. 9, 2021. https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(21)00061-2/fulltext
Pfizer-BioNTech COVID-19 BNT162b2 Vaccine Effectiveness Study - Kaiser Permanente Southern California. https://clinicaltrials.gov/ct2/show/NCT04848584
A PHASE 1/2/3, PLACEBO-CONTROLLED, RANDOMIZED, OBSERVER-BLIND, DOSE-FINDING STUDY TO EVALUATE THE SAFETY, TOLERABILITY, IMMUNOGENICITY, AND EFFICACY OF SARS-COV-2 RNA VACCINE CANDIDATES AGAINST COVID-19 IN HEALTHY INDIVIDUALS. https://clinicaltrials.gov/ct2/show/NCT04368728
Bingham J. Bayer executive: mRNA shots are “gene therapy” marketed as “vaccines” to gain public trust. LifeSite News. Nov. 10, 2021. https://www.lifesitenews.com/news/bayer-executive-mrna-shots-are-gene-therapy-marketed-as-vaccines-to-gain-public-trust/
Bayer pharma exec admits COVID vaccines are “cell or gene therapy”. https://mnfan.org/2021/11/10/bayer-pharma-exec-admits-covid-vaccines-are-cell-or-gene-therapy/
Levine C. Pfizer CEO Alber Bourla calls Israel “world’s lab” in interview to NBC. The Jerusalem Post. Feb. 27, 2021. https://www.jpost.com/breaking-news/pfizer-ceo-albert-bourla-calls-israel-worlds-lab-in-interview-to-nbc-660349
Spiro A. Pfizer exec calls Israel “a sort of laboratory” for COVID vaccines. The Times of Israel. Sept 12, 2021. https://www.timesofisrael.com/pfizer-exec-calls-israel-a-sort-of-laboratory-for-covid-vaccines/